How Infection Control Barriers Impact Dental Curing Light Performance

The COVID-19 pandemic has forced dentists to rethink infection control.
Guidelines on personal protective equipment, cleaning, and disinfection have become stricter than ever and infection control measures have been extended to all of a dentist’s most frequently used equipment.
Take curing lights, which dentist use in more than half of their procedures (1). Infection control barriers were used sporadically before COVID-19, but since the start of the pandemic, they have become essential.
The question dentists should be asking is – does modifying my curing light by placing an infection control barrier on the tip impact its performance?
If it does, it could have a big impact on the success of restorative procedures.
A recent study by Soares, Braga, Ribeiro, and Price (2) explored this topic. In this blog, we summarize their findings and the implications for dentists.
Why infection control barriers are essential
Curing lights play a crucial role in restorative procedures. Because they are used so frequently, they can be handled multiple times a day, in close proximity to multiple patients, which makes them a high-risk area for infection.
Whenever they are used in a patient’s mouth, they are exposed to dental materials that cross-contaminate easily, and are put at risk of cross-infection through blood, saliva, respiratory particles, and viruses.
The Centers for Disease Control and Prevention guidelines categorized light curing units as a semi-critical instrument, for which infection control is essential:
“The use of protective infection control barriers on such devices has become essential to avoid transmitting diseases such as Hepatitis B, Acquired Immune Deficiency Syndrome, and, more recently, COVID-19".
Since curing lights cannot be sterilized, disposable infection control barriers (ICBs) are the most common solution.
They are convenient, non-invasive, and prevent contact between the oral tissues and the curing light. They can also prevent contamination of the light tip with uncured resin.
A 2018 study in Germany found that less than a third of dental offices used disposable infection control barriers (3), but it’s predicted that use of ICBs has increased significantly with the spread of COVID-19.
In our own database of dentists using our CheckMARC service, we’ve seen a 20% increase in curing light tests completed with an infection control barrier in place (4).
But there’s more to consider than just using an ICB or not. There are different types of infection control barrier, which have different designs and use different materials.
How do you know which type to use? And do they impact curing light performance differently?
Do infection control barriers impact curing light performance?
When resin sticks to the tip of a curing light – which is estimated to happen in 35-68% of LCUs in dental offices (5) – it can reduce the light’s output and negatively impact its ability to polymerize composite materials.
So it should come as no surprise that covering your light for infection control purposes can also affect its performance.
A recent study, Effect of infection control barriers on the light output from a multi-peak light curing unit, has investigated how much impact infection control barriers really have.
The study tested a high-powered, multi-wave LED curing light with six different, commercially available ICBs to see what their impact was on various parameters of the light’s output.
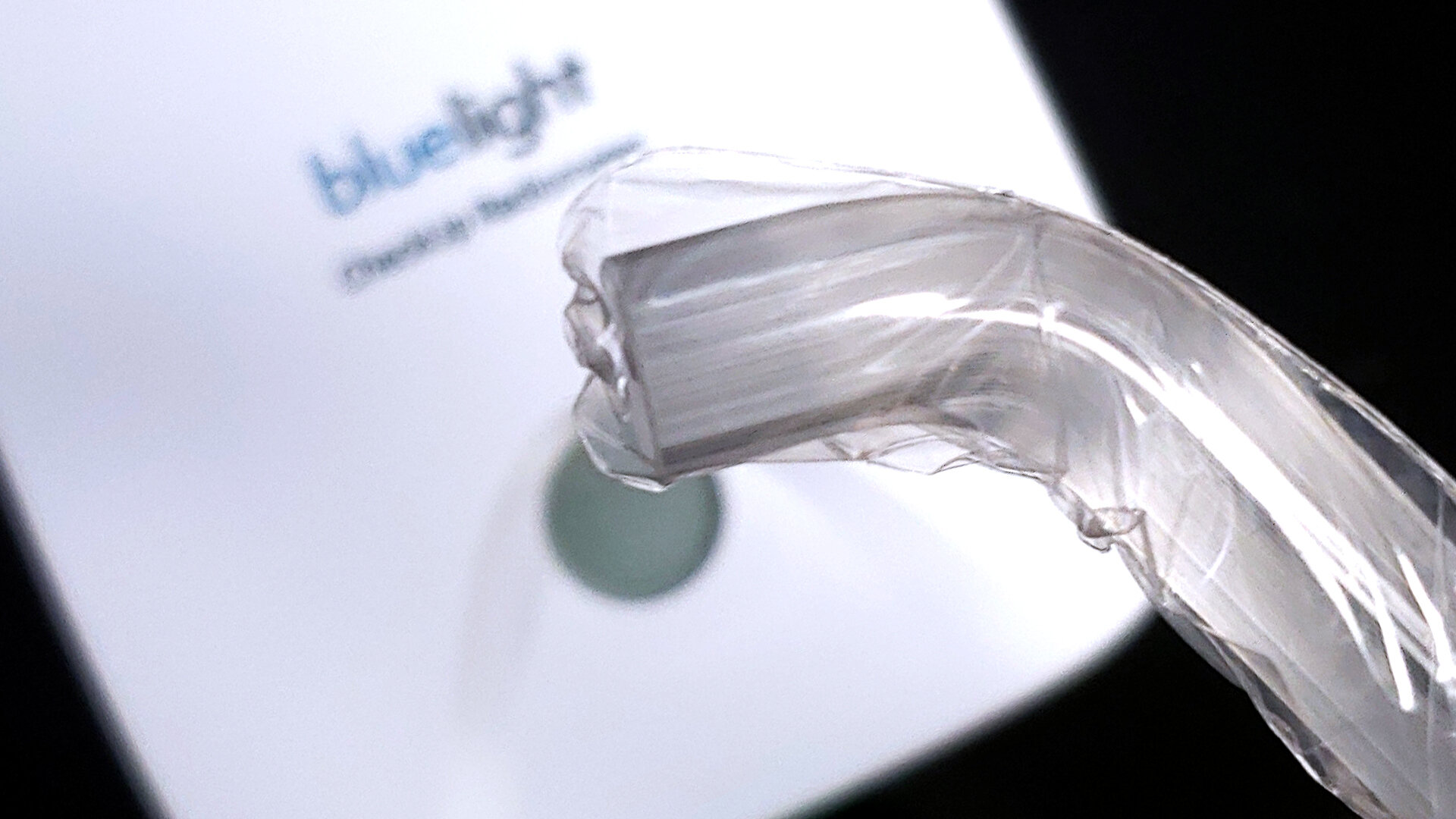
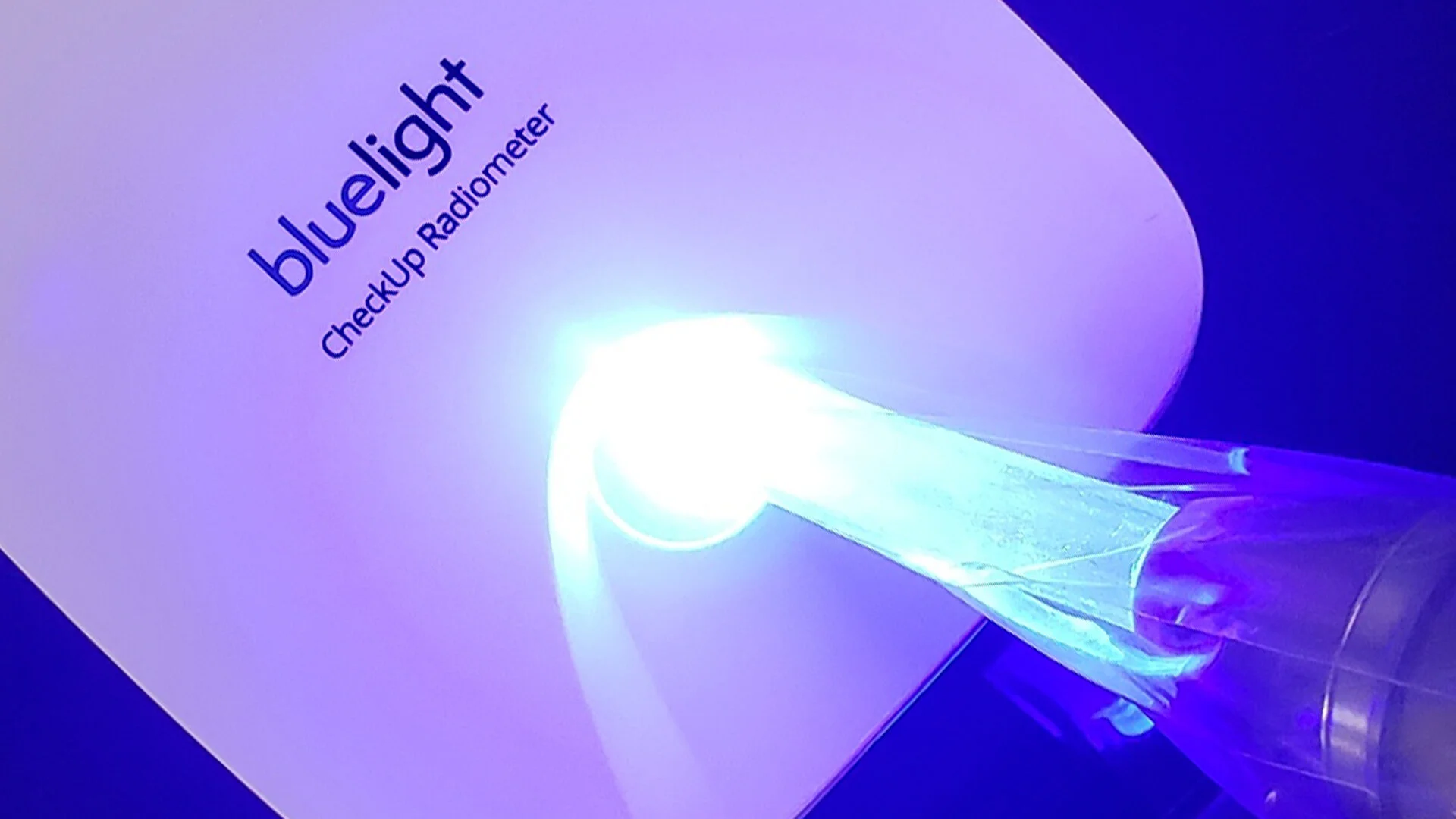
All were tested when positioned correctly – with a smooth transparent face placed over the LCU tip – then again with several different incorrect placements (with seams or opaque sides obscuring the light tip). This was intended to simulate real life situations in a busy dental office.
The study measured and analyzed the light’s radiant power, irradiance, emission spectrum, and beam profile in each situation.
What they found was that regardless of placement or barrier type, infection control barriers significantly reduced the radiant power emitted by the curing light by 5-16%.
The study also showed that infection control barriers impact light performance more significantly when they are applied incorrectly.
When implemented incorrectly, the barriers tested were shown to lower light output by up to 26%.

Examples of incorrect and correct placements of an infection control barrier on a curing light
Here’s what else the study found:
The worst incorrect usage of the ICBs tested was a wrinkled surface of the barrier. This reduced radiant power by 14-26% across all six types of barrier
Polyethylene and polyvinyl chloride-based barriers had less impact on light performance than the one latex barrier tested
Implications for dentists using infection control barriers
The findings from this study are significant for dentists. They suggest that if you’re using an infection control barrier with your curing light – which is highly recommended – you are likely to be applying less power than normal to your composite materials.
And if you’re placing the infection control barrier incorrectly, the light energy you’re applying to your materials could be even less.
If you don’t know the exact output of your curing light and adapt your curing times accordingly, you risk undercuring your materials and compromising your restorations.
How dentists can use ICBs and cure safely and effectively
Dentists are faced with a difficult situation. Infection control barriers are necessary to reduce the risk of contamination and infection. At the same time, they are likely to decrease the output of a curing light, increasing the risk of incomplete curing.
But there are steps dentists can take to overcome this problem.
First and foremost, dentists should ensure that when they use an ICB, they choose one that fits their curing light, then place it carefully, with no folds, seams, or wrinkles over the tip.
Even more importantly, dentists should test their curing lights. Testing your light regularly, both with and without an infection control barrier in place, will tell you exactly how it’s performing, and how much its output changes.
No matter which light or infection control barrier you’re using, if you know how much energy your light is emitting, then you can adapt your curing technique for better patient outcomes.
Here’s are the steps Soares, Braga, Ribeiro, and Price suggest that dentists take to cure safely and effectively:
Our CheckUp radiometer and app make steps 3, 4, and 5 easy.
CheckUp provides you with optimal curing times for your materials by accurately measuring the output of your curing light, with or without infection control barriers.
So whatever light, material, and ICB combination you choose, you can be confident that you’re giving your restorations the best chance of success.

(1) Kevin Frazier, Ana K. Bedran-Russo, Nathaniel C. Lawson, Jacob Park, Sharukh Khajotia, Olivia Urquhart, Dental light-curing units: An American Dental Association Clinical Evaluators Panel survey, The Journal of the American Dental Association, Volume 151, Issue 7 (2020)
(2) Soares, Carlos & Braga, Stella & Ribeiro, Maria & Price, Richard, Effect of infection control barriers on the light output from a multi-peak light curing unit. Journal of Dentistry. 103. 103503 (2020)
(3) C.P. Ernst, R.B. Price, A. Callaway, A. Masek, H. Schwarm, I. Rullmann, B. Willershausen, V. Ehlers, Visible light curing devices - irradiance and use in 302 german dental offices, J. Adhes. Dent. 20 (2018)
(4) Data from Bluelight’s CheckMARC service. Comparison of curing light tests indicating use of an ICB in the period Jan 2018 - Jan 2020 (pre-pandemic) and Oct-Dec 2020 (mid-pandemic)
(5) B.A. Mitton, N.H. Wilson, The use and maintenance of visible light activating units in general practice, Br. Dent. J. 191 (2001)